Altitude Sickness in Mountain – Before hiking in Nepal, it is crucial for you to understand how to prevent altitude sickness also known as Acute Mountain Sickness (AMS), as well as how to cure it if it strikes. Acute Mountain Sickness is a condition brought on by elevation rise. The amount of oxygen is lower at higher altitudes than it is at sea level, and it gets thinner as hikers go further. Please check over the information we’ve provided here about AMS.
There are several possible AMS symptoms. From person to person, they differ. However, the following are general Altitude Sickness symptoms. Do not wait to diagnose the condition and seek prompt treatment if you have any of these symptoms.
High Altitude Pulmonary Edema (HAPE) or HACE may develop in severe cases of AMS (High Altitude Cerebral Edema). The respiratory system is affected by HAPE, whereas the nervous system is affected by HACE.
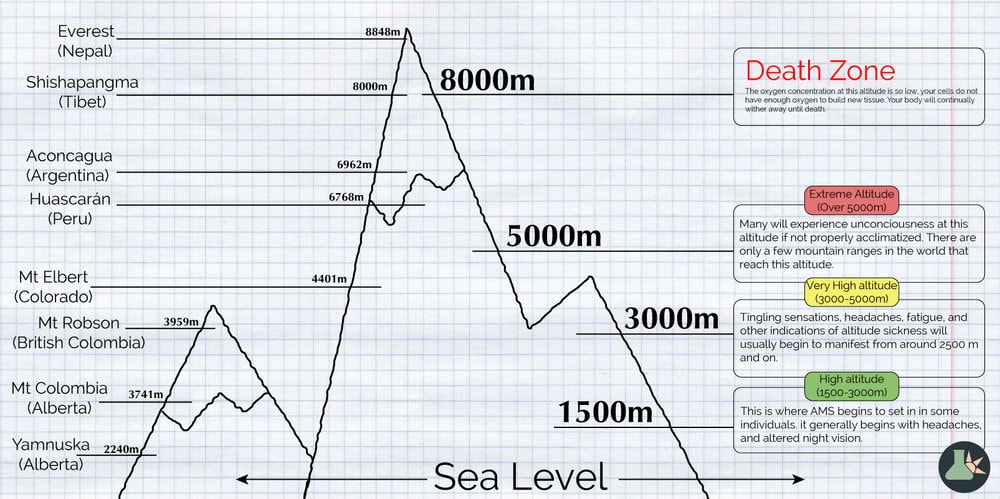
Altitude Oxygen Rate
(In Meters) (In Feet)
8.850 29.035 33%
8.000 26.247 36%
7.000 22.966 41%
6.000 19.865 47%
5.500 18.045 50%
5.200 17.061 52%
5.000 16.404 53%
4.500 14.764 57%
4.000 13.123 60%
3.500 11.483 64%
3.000 9.843 68%
Sea Level 100%
A buildup of fluid in or near the brain is what causes HACE. Typically, AMS symptoms and indications worsen and HACE manifests. HACE could develop in a person with HAPE.
Walking Test: The subject is instructed to take 10 extremely little steps while stepping from the heel of one foot to the toes of the other. The victim shouldn’t be assisted, and the terrain ought to be quite flat.
Standing test: The subject stands with their feet together, their arms at their sides, and their eyes closed.
Finger – Nose Test: The subject closes their eyes and swiftly alternates between tapping the tip of their nose with the index finger and extending that arm to point in the opposite direction. This is known as the “finger-nose test” (a useful test if the victim is in a sleeping bag).
Mental Arithmetic Test: Give the sufferer a mental calculation test, for instance. 7 should be subtracted from 100, 7 from 93 (but remember some people may be poor at arithmetic even at sea level).
Assume the victim has HACE if they are unable to complete any of the aforementioned tests without assistance (or if they refuse to cooperate), exhibit excessive wobbling, or trip over during the first two tests (be ready to catch the victim if they fall over!). Compare the victim’s performance to that of a healthy person if you are unsure. Be ready to take these tests repeatedly.
Drop instantly (prompt descent will begin to reverse the symptoms). Get as low as you can, at least 1000 meters (3280 feet). If necessary, descend at night or during terrible weather.
Oxygen or the use of a PAC together with the required drugs will keep the individual alive until descent can be started if descent is not immediately possible (due to hazardous terrain or weather, a lack of rescuers, or while waiting for a helicopter, for example).
Note: If a pressure bag and oxygen are both available, use the oxygen first while the victim is being readied for the bag and then again once they are removed. If the bag is not intended for this use and you have not received training to do so, do not administer oxygen within the bag.
The person should be supported in a semi-reclining position because lying flat could worsen their condition.
If at all possible, refrain from making even the smallest effort. Even a brief walk could exacerbate or bring back their symptoms. Don’t let the victim be left alone.
Give someone rescue breathing if they are going blue or are about to lose consciousness before they cease breathing.
The buildup of fluid in or around the lungs is what causes HAPE. It may develop concurrently with AMS or it may manifest on its own without any prior AMS symptoms (this occurs in roughly 50% of cases). If in doubt, treat for both asthma and a chest infection since HAPE is easily confused with either condition.
Dry coughing and a decline in physical function are sometimes the first indications that HAPE is beginning to experience dyspnea.
This may just include taking a little longer to breathe while returning to rest after little exertion in the early stages of HAPE. Later, even light exertion causes noticeable dyspnea. Finally, being at rest causes dyspnea. Take note of your breathing rate.
Later on, the dry cough could turn wet and produce frothy, bloody sputum (pink or rust colored). This is a grave indication.
Deep breathing produces wet sounds in the lungs (place your ear on the bare skin of the victim back below the shoulder blades; compare with a healthy person).
Be aware that even in very severe cases of HAPE, there may be NO wet noises; this is known as dry HAPE.
Mild temperature up to 38.5oC, a feeling of inner chill, and chest aches are possible.
due to a shortage of oxygen in the blood, you may have blue or dark skin, lips, tongue, or nails (cyanosis).
Use oxygen or the PAC and the needed drugs to keep the person alive until descent can be attempted. Otherwise, use the same general course of action as for HACE.
